Pyloric Stenosis Overview:
Pyloric stenosis is a common cause of persistent vomiting in infants during their first weeks of life.
It typically presents between 2 and 8 weeks of age but can appear as late as 12 weeks.
The exact cause is unknown, but genetic and environmental factors are believed to play a role.
Males are more commonly affected than females.
The hallmark symptom is projectile, non-bilious vomiting.
Bile in the vomit rules out pyloric stenosis as the cause.
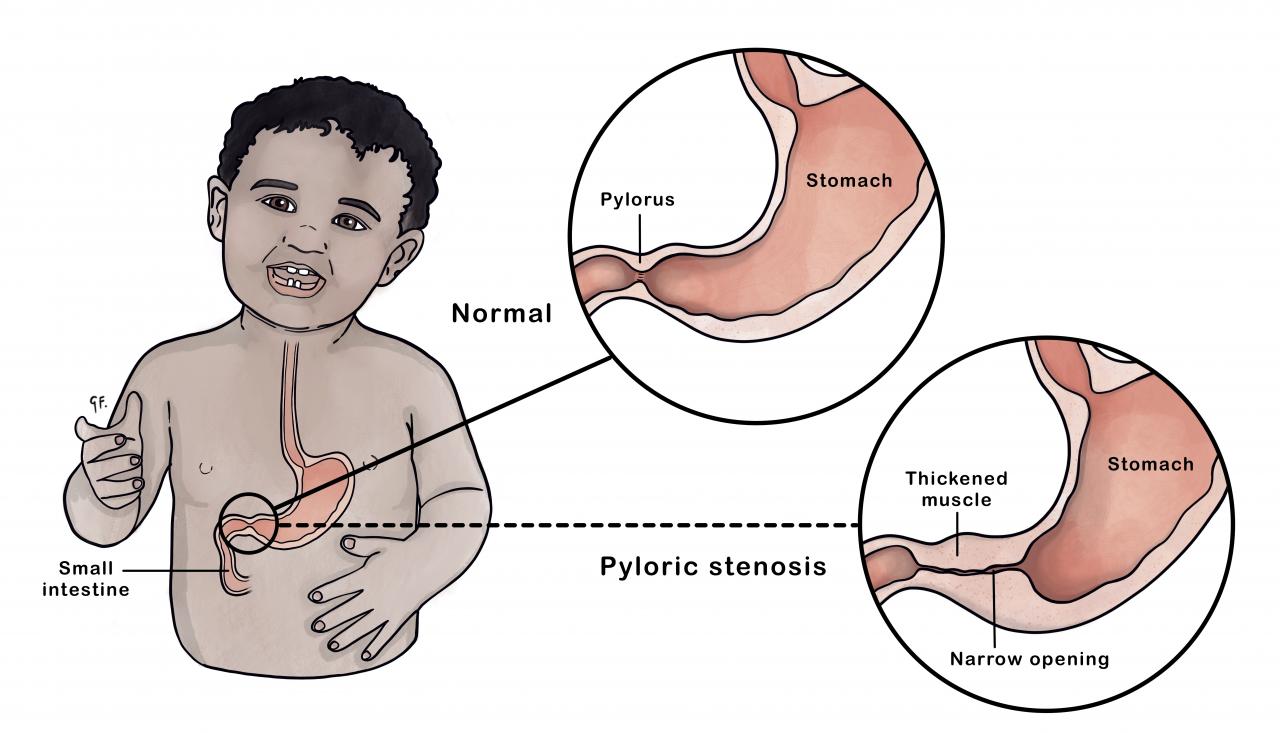
.png)
Definition:
Hypertrophic pyloric stenosis (HPS) results from thickening of the pyloric muscles, narrowing the pyloric canal.
It’s the most common surgical cause of vomiting in infants.

Symptoms:
Progressive projectile vomiting after feeding (typically non-bilious).
An upper abdominal mass or visible gastric wave may or may not be present.
Untreated vomiting can lead to dehydration, hypochloremia, hypokalemia, and metabolic alkalosis.
Epidemiology:
More common in males and firstborn children.
Lower incidence in African and Asian populations.
Differential Diagnosis:
Consider other conditions like overfeeding, gastroesophageal reflux, malrotation, duodenal stenosis, and intracranial lesions.
Management:
Suspected Pyloric Stenosis:
1. Perform a basic metabolic panel (BMP).
2. Ensure the patient is nil per os (NPO).
3. Administer a Normal Saline bolus.
4. Conduct a pyloric ultrasound.
5. Consider repeat ultrasound or upper GI contrast study if inconclusive.
Confirmed Pyloric Stenosis:
1. Consult with pediatric surgery.
2. Review serum electrolyte results.
3. Place a nasogastric tube.
4. Monitor the infant closely.
Emergency Considerations:
Pyloric stenosis is a medical emergency.
Correct electrolyte imbalances before surgery.
Rehydration protocols depend on clinical condition.
Inpatient Management for Pyloric Stenosis:
Pre-Surgery:
Ensure the patient is fully hydrated and correct electrolyte imbalances.
Surgical intervention (pyloromyotomy) is necessary.
Pyloromyotomy can be performed openly or laparoscopically.
Post-Surgery:
Feeding can resume within two hours after the procedure.
Pain management with Tylenol only.
Feeding regimen at the discretion of the attending physician (usually breastmilk or Enfamil).
Some initial vomiting is common; parents should be reassured unless advised otherwise.
Discharge:
Expect discharge on postoperative day (POD) 1 or 2.
Documentation Recommendations:
Document any electrolyte or acid-base abnormalities.
Note presence and severity of dehydration at admission.
Document shock status at admission.
Note: Always follow your hospital protocol for managing patients with pyloric stenosis
References:
Dalton BG, Gonzalez KW, Boda SR, Thomas PG, Sherman AK, St Peter SD, Optimizing fluid resuscitation in hypertrophic pyloric stenosis. J Pediatr Surg. 2016 Aug; 51(8):1279- 82
Jobson M, Hall N, Bchir MB, Contemporary management of pyloric stenosis. Seminars in Pediatric Surgery 2016 Aug; 25(4):219-224.
Markel TA, Scott MR, Stokes SM, Ladd AP, A randomized trial to assess advancement of enteral feedings following surgery for hypertrophic pyloric stenosis. J Pediatr Surg. 2017 Apr;52(4):534-539


{kind=link}
No comments:
Post a Comment