Fall Prevention and Management
DEFINITIONS: Fall - A patient fall is a sudden, unintentional descent, with or without injury to the patient, which results in the patient coming to rest on the floor, on or against some other surface (e.g., a counter), on another person, or on an object (e.g., a trash can or other equipment). It includes falls resulting from physiological and environmental factors as well as assisted falls resulting from physiological and environmental factors as well as “assisted falls”.
When a patient rolls off a low bed onto a mat or is found on a surface where you would not expect to find a patient, this is considered a fall. If a patient who is attempting to stand or sit falls back onto a bed, chair, or commode, this is only counted as a fall if the patient is injured.
Observed Fall is a fall in which any staff member, nursing personnel or not, observed the patient’s fall. Unobserved falls include any case when a staff member finds the patient on the floor or other surface or when a fall is reported by the patient, a family member, or visitor.
FALL PREVENTION BUNDLE Patient falls occurring during hospitalization can result in serious and even potentially life threatening consequences for many patients. Nurses are responsible for identifying patients who are at risk for fall and for developing a plan of care to minimize that risk. The fall prevention bundle is a set of evidence based interventions and practices aimed at reducing the risk of falls that outlines practices that must be adhered to for every patient every time to ensure patient safety and high quality care. The fall prevention bundle aims to achieve a fall rate less than the national benchmark of 3.4% through a multifaceted fall prevention program that includes staff education, patient assessment, ongoing monitoring and improvement initiatives.
Nursing education for RNs and ancillary team members begin at onboarding. Periodic education is provided through unit huddles, clinical updates, learning management system, debriefings, and individual/team coaching. Annual review is required for all team members of the fall prevention bundle.
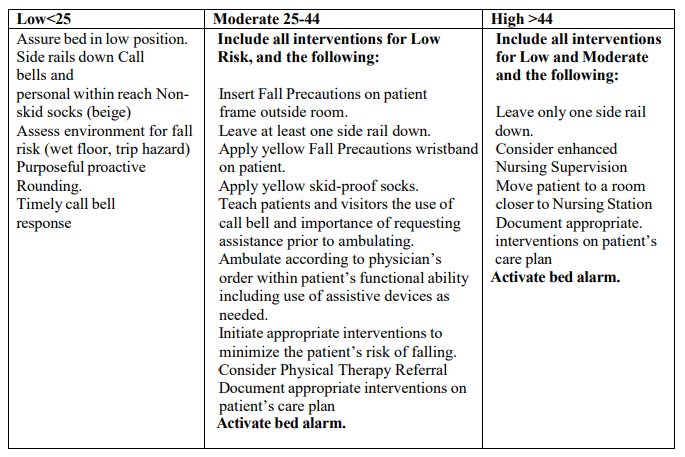
Morse Fall Scale for adults and the Humpty Dumpty Scale for Pediatrics (birth to 17-years of age) is the adopted assessment for the hospital used to identify fall risk factors than can support developing an individualized care plan for the patient. This assessment is completed at the point of entry (ED Triage), Main ED, every shift, upon transfer, and if there is a change of condition. The scale quantifies the patient risk that indicates if the patient risk for fall is low <25, moderate <25- 44, and high >44. Each level of risk warrants a set of interventions. Once the assessment is complete, interventions are selected, and the plan is tailored to the patient.
• Room Signage
• Yellow Gown
• Side rails down
• Patient and family education
• Nonskid Socks
• Bed in its lowest position
• Call Bell within reach
• Enhanced nursing supervision
• Fall Risk Band
• Assess environment for risk
• Yellow Nonskid socks
• Activate bed alarm
• Physical therapy referral
• Ambulate according to physician’s order
Purposeful rounding is a proactive and systematic approach that helps anticipate and address patient needs such as addressing the 4Ps (pain, personal needs, position and placement.
Continuous video monitoring is effective in reducing patient fall and other patient concerns with real-time video rather than video recording to protect the patient’s privacy. (See Continuous Visual Monitoring for Patient Safety Using the Avasys Telesitter Solution Policy)
Bed Alarms- reduce falls by alerting the patient care team that the patient is attempting to move.
Fall Debriefings are conducted for reflection and learning, continuous improvement, enhanced communication, psychological support and decision making playing a crucial role in promoting a culture of learning, accountability and continuous improvement within the organization.
Fall Committee is an interdisciplinary approach that over sees fall prevention initiatives through monitoring and evaluating the effectiveness of fall prevention efforts that includes reviewing the data on fall rates, root cause analysis for incidents, and identifying areas for improvement; facilitates collaboration and communication among different departments and disciplines.
Patient and family education is crucial for promoting safety and reducing the risk of falls. The care team should review fall precautions implemented, discuss and identify potential side effects or interactions that could increase the risk of falls, orientation to the room that includes equipment, and routine checks. The team should validate that the patient understands through the methods such as the teach back method.
Interventions based on Morse Scale (may exceed required low interventions, but never lower at the nurse’s discretion)
Patient education • Nurses will educate patients and their families about fall prevention techniques, including proper use of assistive devices, the importance of calling for assistance, and purposeful proactive rounding.
Documentation • The nurse must document in the medical record the patient’s level of risk for fall/injury and level of intervention implemented and strategies, and patient/family education. • Refusal for intervention: The nurse must document date and time of refusal, description of the intervention, reason given by the patient for refusing, any attempts made to encourage the patient to accept the care, risks and consequences explained to the patient, and the patient’s understanding of the refusal and its implication.
Ongoing Risk Assessment 1. The nurse will complete the Fall Risk assessment with shift assessments, at transfer, after a fall and/or with a functional change in patient condition. 2. If patient condition/score changes, or at the nurse’s discretion, Fall Precautions may be initiated or discontinued. 3. All patients who have had a lower extremity nerve block anesthetic will be automatically placed on Fall Precautions until the nerve block is discontinued. The patient will then be reevaluated to determine his/her fall risk.
Fall Management (following a reported or observed fall) Immediate Response
1. If a patient experiences a fall, if possible, do not move the patient until an assessment of potential for serious injury can be made.
2. Obtain vital signs prior to the patient being moved.
3. Assess level of consciousness
4. Assess movement of extremities
5. Notify Physician.
6. Document in the nurse’s progress notes including patient appearance at time of discovery, patient response to event, evidence of injury, location, medical provider notification, medical/nursing actions.
• Reassess for fall risk after the patient is returned to bed; as risk level may be upgraded.
• Update fall prevention interventions based on post-fall assessment
Physician Notification
1. The responding physician will perform a post fall patient assessment and document results in medical record.
2. Physician will order any imaging or interventions as indicated.
3. If a radiology test is ordered, as a result of the fall, the results should be reviewed within 2 hours of the fall. Further treatment, if necessary, will be determined based on the results.
4. The responding physician will notify the patient’s family.
5. Update interventions if changes are noted in the patient’s condition.
6. Physician will document interventions, results, and notifications in record.
Reporting
1. Inform Risk Management and Nursing Manager/Supervisor immediately.
2. Conduct a Post Fall Huddle as soon as possible after the fall. The Nurse Leader (Manager/Director/Supervisor/ANM) will lead the post fall huddle. This should include the charge nurse, RN, LPN and NA involved in the patient’s care. The patient and/or family member may be included in the huddle.
3. Complete Post Fall Debriefing/Investigation review form with the involved staff from the post fall huddle and forward the completed form to Nurse Manager and Risk Management Department.
4. Communicate in shift handoffs that the patient has fallen and is placed on high-risk protocol. 5. Complete a Fall Incident report in Meditech Risk Management Module.
6. Nurse Manager to complete Corrective Action section in the EMR.
7. Risk Management is to complete the final injury level.
Classification of Severity of Injury
1. None - Patient had no injuries (no signs or symptoms) resulting from the fall; if an x- ray, CT scan or other post fall evaluation results in a finding of no injury
2. Minor - resulted in application of dressing, ice, cleaning of a wound, limb elevation, topical medication, pain, bruise or abrasion.
3. Moderate - Resulted in suturing, application of steri-strips/skin glue, splinting, or muscle/joint strain.
4. Major - Resulted in surgery, casting, traction, required consultation for neurological (basilar skull fracture, small subdural hematoma) or internal injury (rib fracture, small liver laceration) or patients with coagulopathy who receive blood products as a result of a fall.
5. Death - The patient died as a result of injuries sustained from the fall (not from physiologic events causing the fall)
External Reporting
1. Risk Management will review falls sustaining major injury or death for reporting as per NYS DOH NYPORTS requirements.
2. A root cause analysis is performed to identify and remediate contributing factors when possible
Fall Prevention Program Evaluation:
1. The Fall Prevention Committee will review incident reports, post fall debriefing/investigation forms and summary reports to identify patterns/concerns and to determine the need for corrective action and further monitoring.
2. Information from this committee will be reported to the Hospital Performance Improvement Committee on a quarterly basis.
RELEVANT REFERENCES:
1. AHRQ Fall and Safety Guidelines:https://www.ahrq.gov/professionals/systems/hospital/fallpxtoolkit/fallpxtktool3i.html
2. Preventing falls in hospitals. (2023). Agency for Healthcare Research and Quality. www.ahrq.gov/patient-safety/settings/hospital/fall-prevention/toolkit/index.html
3. Press Ganey (January 2023). NDNQI patient falls indicator.
4. Safe Sleep https://www.aap.org/en-us/advocacy-and-policy/aap-healthinitiatives/child_death_review/Pages/Safe-Sleep.aspx
5. Prevention of in Hospital Newborn Falls-https://doi.org/10.1111/j.1751-486X.2011.01611.x
6. The Joint commission of Quality and Safety-https://doi.org/10.1016/j.jcjq.2018.12.001 https://www.jointcommission.org/standards/national-patient-safety-goals/hospital-nationalpatient-safety-goals/


No comments:
Post a Comment